We speak with clients all of the time who are facing challenges justifying the investment in personnel and software support required to start, run, or grow their cancer genetic counseling and high risk programs.
In this post, we’ll teach you how to forecast the ROI of your cancer genetics or high risk program so you can get resources for the people, tools, and processes needed for success. We'll discuss:
- Source Data and Basis for Our ROI Methodology
- 3 Levers of ROI
- Increasing Patient Volume
- Decreasing Per Capita Cost (Increasing Profitability)
- Generating Incremental Downstream Revenue
- Resources to Generate Your Own ROI Forecast
Source Data and Basis for Our ROI Methodology
The team at CancerIQ is extremely data-driven, and has benchmarked both clinical, operational, and financial outcome data across the dozens of hospital systems that work with us. To understand the source of the case studies and figures presented in our analysis, here is the data set we are working with:
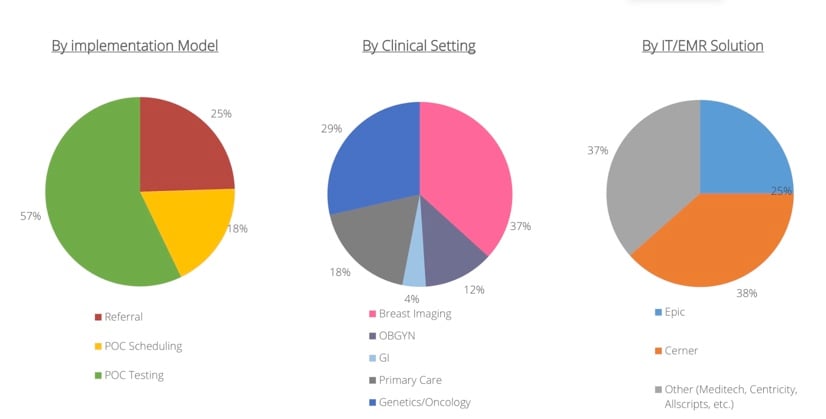
Diverse Clinical Environments
Our track record comes from implementing CancerIQ in a diverse range of clinical environments. Our clients have chosen different implementation models, deployed CancerIQ in a broad range of clinical settings, and have operated CancerIQ alongside a diverse range of existing HIT systems.
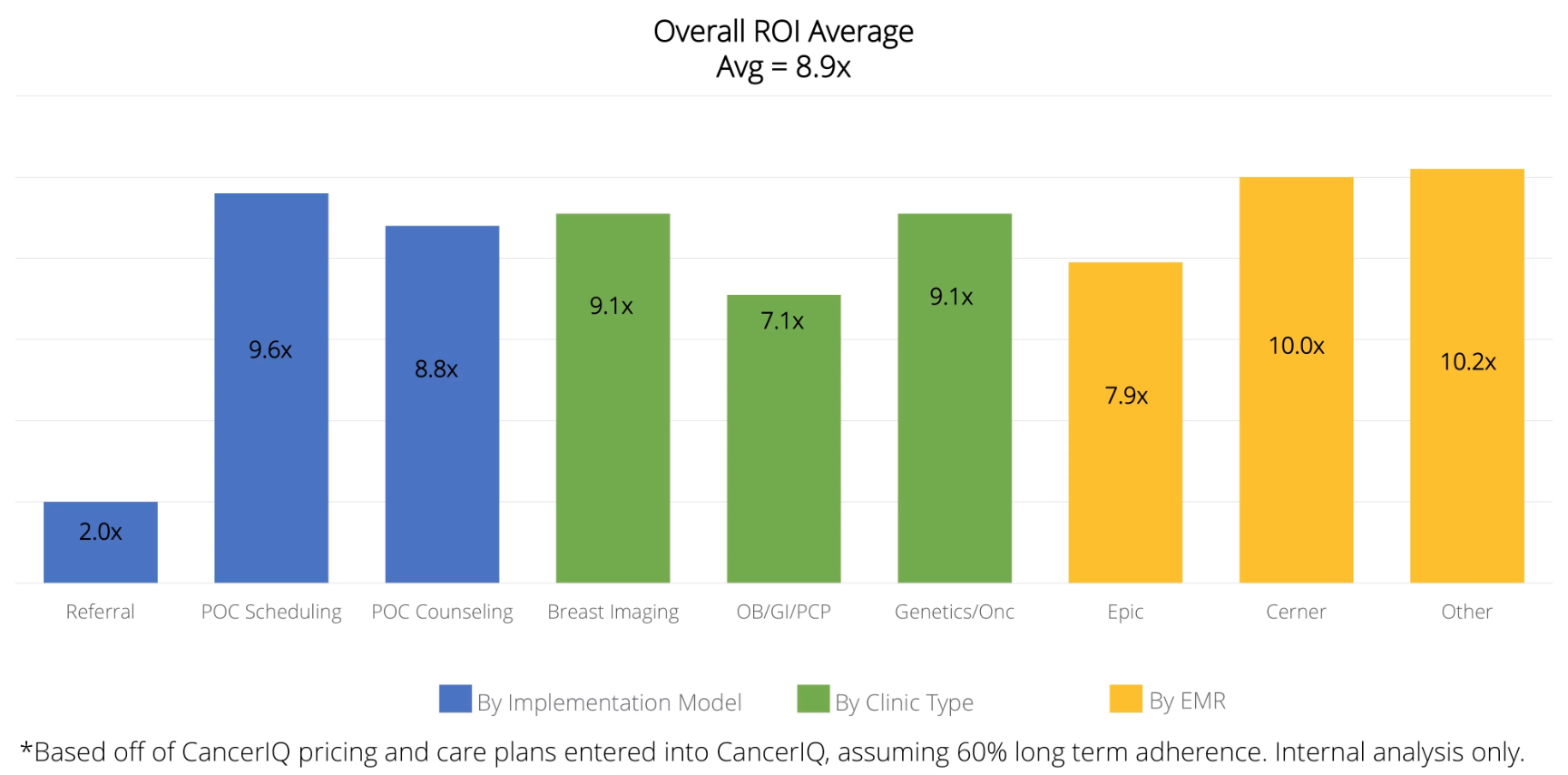
Consistently High ROI
Despite the diverse clinical settings we operate in, the fundamental drivers of ROI are the same. And when applied across our health system clients - we have seen consistently high ROI across nearly all of our client categories.
Key Sources of Value from Your Cancer Risk Assessment Program
First off, when determining the ROI, it’s important to look at these three categories:
- Increasing patient volume
- Improving profitability by decreasing service delivery costs
- Generating downstream revenue
We’ll take a look at each one of these areas and provide a few examples from our clients showing how they turned their program into a source of revenue for the health system (with a little help from CancerIQ).
ROI Lever #1: Increasing Patient Volume
Identifying patients eligible for genetic evaluation services is at the top of the funnel, and the first lever to pull to generate an ROI on your high risk program
[Case Study] Identifying More High Risk Patients at Marin General
One of our clients, Marin General Hospital, started their program using the Tyrer-Cuzick score embedded in their radiology information system.

- The Challenge: The patients referred to the genetics-trained provider were often inappropriate candidates for genetic testing, meaning that patients that could be seen by someone with less expertise. Only 46% of patients seen received genetic testing.
- The Change: To solve this challenge, Marin launched a CancerIQ screening process in parallel to the risk assessment process in their radiology information system. As suspected, Marin found that 19% of patients identified using the NCCN guidelines in CancerIQ would have been missed using their old system.
- The Impact: The impact at Marin on a broader scale was demonstrable. Not only did the enhanced screening criteria result in more patients being identified, but it led to a more appropriate use of their highly valued genetic specialist. The program grew 3.9x from 139 patients the year prior, to 521 patients after implementation of CancerIQ.
ROI Lever #2: Decreasing service delivery costs (and increasing profitability)
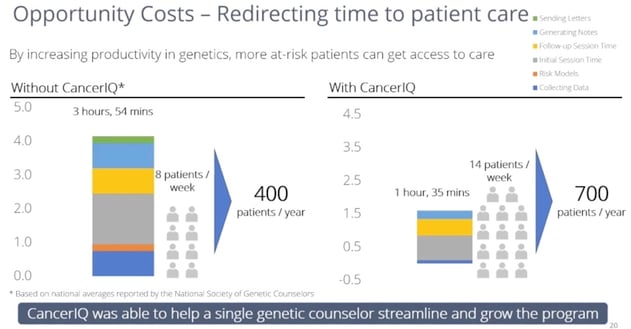
According to the National Society of Genetic Counselors, an average genetic counselor sees 10 patients per week. Unlike other medical professionals, they have triple the documentation burden (generating notes for patients, providers, and insurance companies), and they spend a lot of time gather data using interview-based techniques. Based on time studies observed in dozens of practices across the country - these non-clinical tasks are the primary cause for constraints in genetic counselor capacity.
[Case Study]: Increasing Visit Capacity at Advocate Illinois Masonic
- The Challenge: At AdvocateAurora Health, the cancer center leadership needed to have on site genetic counseling resources to keep up with competition for the large academic medical centers in town. Even though timely access to genetic counseling was the best way to prevent leakage to other comprehensive cancer programs in the city, Advocate Illinois Masonic needed to find a way to meet patient demand with a single genetic counselor resource.
- The Change: After experiencing turnover in genetic counseling staff, the leadership at the cancer center decided to invest in infrastructure needed to attract and retain a genetic counselor. This included providing clinical support services (a scheduler and medical assistant), and investing in cancer genetic counseling software. The goal was to increase genetic counseling productivity without burning their genetic counselor out.
- The Outcome: The genetic counselor at Advocate Illinois Masonic was able to cut down on the time spent gathering family history information, producing documentation for genetic test order, and generating letter for multiple stakeholders involved in the broader care team. She could double the number of appointment slots available for patients, and instead focus on the things that were fulfilling for her career - spending time on complex cases, and assuming a clinical leadership role within the organization.
Read insights from Maritess Caamic, Director of the Cancer Institute and Infusion Services at Advocate Illinois Masonic Medical Center in our previous post "10 Cancer Risk Assessment Questions Every Administrator Has"
ROI Lever #3: Generating Downstream Revenue
The greater opportunity with a cancer genetics program is not the direct revenue, but the downstream revenue that comes from the management of patients classified at increased risk. Genetic counselors will recommend a change in medical management for 40% of patients they see, with 10% of patients testing positive, and approximately 30% of patients testing negative for remaining at elevated risk due to familial risk factors. To demonstrate the potential downstream revenue potential, we'll share a case study from a breast center, and from a cancer center's perspective.
[Case Study] Generating Downstream Revenue in a Breast Center-Based High Risk Program
The specific revenue opportunities in a breast center staffed by a high risk nurse practitioner include:
- Breast MRIs
- Clinical Breast Exams
- Prophylactic Mastectomies
The following case study is how one high risk breast program was able to deliver on their promise of downstream revenue
- The Challenge: Many standalone breast imaging centers may include a note in the mammography report about the need for a breast MRI or the need to explore genetic testing. Based on a study done by John Brinton, one mammography clinic saw 64,659 patients screened in their high volume clinic. Collaborating with your affiliate surgical practices to staff your program with a nurse practitioner or PA can increase the likelihood of getting patients to comply.
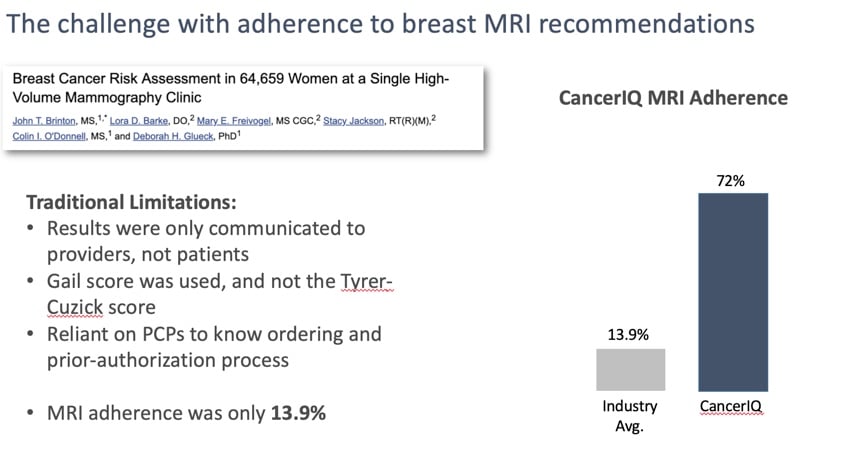
- The Change: Rather than let patients leave the breast center with a light recommendation to pursue high risk services, OSF invested in an in-house program to identify and manage patients at risk. The nurse practitioner could develop a relationship with the patient, order breast MRIs on behalf of their home provider, and ultimately track adherence to medical management recommendations in CancerIQ instead of on spreadsheets.
- The Outcome: Over the 18 month period after implementing CancerIQ, the breast center increased their breast MRI volume 35x from 3 MRIs received prior to CancerIQ to 105 after CancerIQ. And concurrently with the breast MRI appointment, patients can be seen by the nurse practitioner for a clinical breast exam. These procedures and touch points with the NP more than paid for the additional investment in salary and software.
Hear more from Michele Settelmyer, Risk Assessment APN at OSF Healthcare, in our webinar: Implement a Genetic Screening and Navigation Program in an Imaging Center
[Case Study] Generating Downstream Revenue in a Cancer Center-Based Genetics Program
A genetic counseling program within a cancer center has a different set of downstream revenue opportunities than a breast center based program, as they typically serve a broader range of affected and unaffected patients, and make recommendations for management of non-hereditary breast and ovarian cancer conditions. The following case study shares the experience of Sharp Healthcare, whose results were published in the Advisory Board:
- The Challenge: Many cancer genetics programs promise to deliver a return on investment to the cancer program, but struggle to quantify the extent to which they deliver a return on investment.
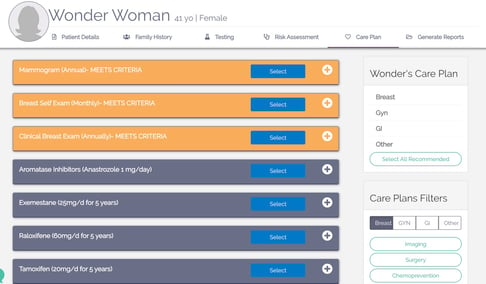
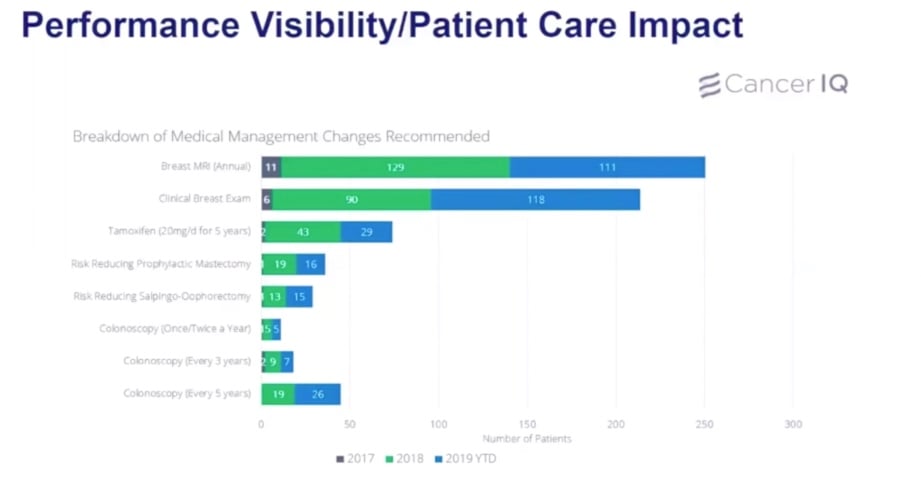
- The Change: Instead of having the genetic counselors spend time logging procedures in a spreadsheet or asking IT analysts to pull procedure data from the EMR, our users are able to generate actionable reports on downstream revenue directly from CancerIQ. The practice of "logging" recommended medical management changes is not a separate activity, it is something that is part of the documentation note generation workflow. Each "click" on a care plan in CancerIQ autogenerates an element of the GC's consultation note, that concurrently becomes part of CancerIQ's analytics services.
- The Outcome: Since converting to CancerIQ, the team at Sharp has been able to provide informative reports to executive leadership about their contributions to other service lines within the Sharp Healthcare system. In several cases, they have also demonstrated that they have prevented over-utilization of services that may not be appropriate.
Read: 8 Key Takeaways from Association of Cancer Executives Webinar: Improving Access to Genetic Counseling and Testing
Resources to Apply to your Own ROI Model
Step 1: Estimate The Volume of Patients Eligible for Genetic Counseling & Testing
As seen in the Marin Case Study, the return on investment in a comprehensive high risk program can depend heavily on the volume of patients at the top of the funnel.
- If you use the Tyrer-Cusick Model as a screening model - expect that approximately 16% of patients will meet high risk criteria and be referred onwards for a genetic evaluation
- If you use a more comprehensive screening tool that includes multiple criteria (NCCN Guidelines, US Preventative Service Task Force Guidelines, ACOG Guidelines, AsBRS Guidelines) - expect that 25% of patients will meet high risk criteria
Step 2: Estimate Your Volume of Genetic Counseling / High Risk Visits
If you have a genetic counselor and are trying to estimate the productivity gains for your organization, assume that the current staff you have offering genetic counseling services will be able to see up to 2x the number of patients within the first year using CancerIQ.
- If you bill for genetic counseling, this will double the direct revenue from your genetic counseling program
- If you don't bill for genetic counseling, this will reduce your genetic counseling delivering costs by 50%
If you don't have a genetic counselor and are trying to estimate the percentage of patients identified that will be seen by a newly formed genetic counseling position, assume that patient uptake will be dependent on the implementation model that you choose. According to our data, patient uptake is:
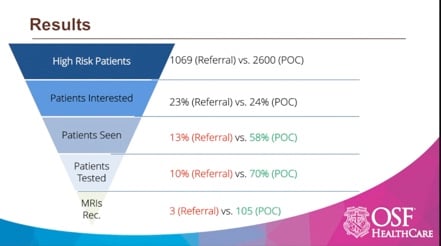
- 70%-80% if you offer point of care counseling
- 35%-50% if you offer point of care scheduling for counseling at a future date
- >10% if you choose to refer the patient for counseling with no follow-up
Step 3: Forecast Your Genetic Counseling & Testing Outcomes
On average, assume that 10% of patients seen by your high risk specialist will test positive, and 30% will test negative.
Step 4: Estimate Patient Medical Management Preferences
For the patients who test positive, assume they will choose the following risk reduction strategies:
- 72% will choose risk reduction methods, with
- 21.3% choosing annual breast MRI [2-4]
- 19.7% choosing Mastectomy w/ Reconstruction [5]
- 35.4% choosing Oophorectomy [5]
- 15.7% choosing Mastectomy & Oophorectomy [5]
- 7.9% choosing Chemoprevention [6]
Step 5: Estimate Patient Adherence
As we've learned from several implementation models, patient compliance with medical management recommendations can vary based on the workflow of your high risk program. If there is not a formal infrastructure in place to follow up with patients and their providers, we have found adherence numbers to be incredibly low. To inform this assumption, we have looked closely at adherence rates pre and post implementation of CancerIQ.
No formal process in place - 80% of patients that test positive will comply, but only 25% of high negatives may comply with their medical management plan.
Software-enable process: 85%-90% of patients that test positive will comply, and 60% of high risk negatives will comply. Through ongoing patient reminders and visual queues for the provider to act on
Step 6: Identify One-Time and Recurring Sources of Revenue
While certain procedures are one-time events, the majority of patients with a high risk diagnosis are going to be on a high risk surveillance plan for the rest of their lives. This means that your ROI will not only be driven by revenues generated on a one-time basis, but for years to come.
If your institution is preparing to shift from fee-for-service to fee-for-value, it is critical to think through these financial matters so you're prepared for the change in business model.
Because what does this mean in practice? It's time to act now and invest in stratifying your patient population as soon as possible. You will want to complete all the costly risk reducing procedures before value based contracts kick in. You will want to know how many high risk patients will need high risk surveillance services before negotiating bundled payments for your population.
Here's the good thing - developing a hereditary cancer risk assessment program is a win-win in all healthcare business model. Mutation carriers are typically at risk for extremely costly, early onset cancers - and implementing a hereditary cancer screening program to avoid those cancers will help prevent those outlier cases down the line.
If your head is spinning after this article and you need some help calculating an ROI and making the case for your program, we're here to help.
Click below to access a member of our team and our ROI calculator.

References
[1] Rosenthal et al. Outcomes for Clinical Testing on 76,000 Patients Using a Panel of 25 Genes Associated with Risk of Breast, Ovarian, Colorectal, Endometrial, Gastric, Pancreatic, Melanoma, and Prostate Cancers. Abstract 1515 Presented at ASCO, June 2015
[2] Plevritis SK, Kurian AW, Sigal BM, et al. Cost-‐effectiveness of screening BRCA1/2 mutation carriers with breast magnetic resonance imaging. JAMA : the journal of the American Medical Association. May 24 2006;295(20):2374-‐2384.
[3] Warner E, Plewes D, Causer P, et al. Effect o Age and Temporal Patterns Over 5 years in a magnetic resonance imaging (MRI)-‐based Breast Surveillance Study for BRCA Mutation Carriers. ASCO Annual Meeting; 2004; New Orleans.
[4] Consumer price index-‐medical care, all urban consumers (US city average, not seasonally adjusted) http://data.bls.gov/cgi-‐bin/print.pl/news.release/cpi.nr0.htm. Accessed Dec 5th, 2016.
[5] Grann VR, Patel PR, Jacobson JS, et al. Comparative effectiveness of screening and prevention strategies among BRCA1/2-‐affected mutation carriers. Breast cancer research and treatment. Feb 2011;125(3):837-‐847.
[6] Red Book Pharmacy's Fundemental Reference. Montvale, NJ: Thomson PDR; 2008.