When implementing a hereditary cancer risk assessment program into routine care, the goal is simple: Provide genetic counseling and genetic testing to all high-risk patients. In doing so, healthcare providers can better predict, preempt, and prevent cancer across their patient populations before a diagnosis. The success of any risk assessment program depends on how many high-risk patients meet with your genetic counselor and receive appropriate changes in their medical management based on genetic risk factors.
However, according to a comparison of observational data by faculty associated with City of Hope, University of Illinois at Chicago, and the University of Chicago Medicine, how you implement your cancer risk assessment program can impact the success of patient uptake.
There are three main ways to implement a hereditary cancer risk assessment program:
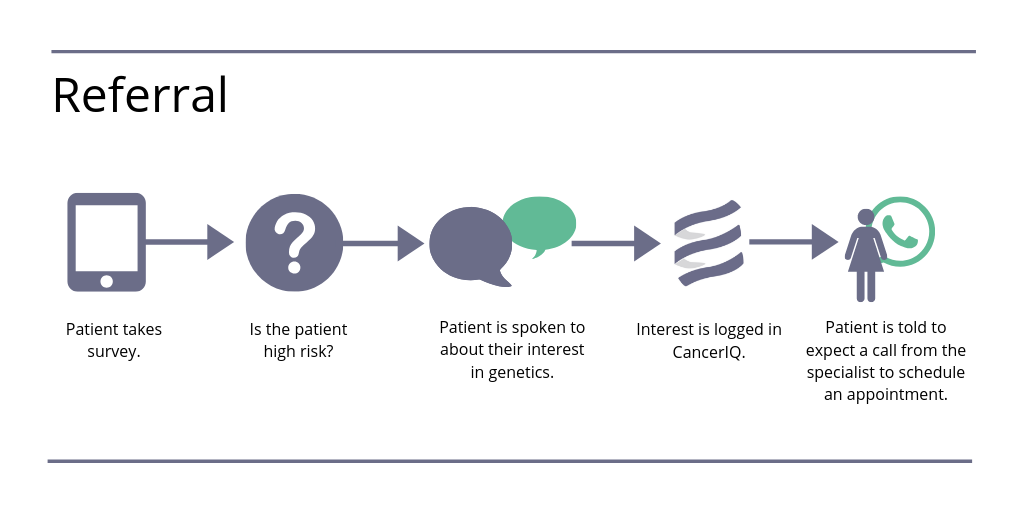
(1) The referral model. In this model, the screening site refers high-risk patients who are interested in genetic counseling to a genetic specialist. The patient leaves the facility with no concrete next steps, but is contacted at a later date and time to schedule an appointment with the specialist. Or in some cases, the patient is expected to call the genetic specialist to schedule an appointment.
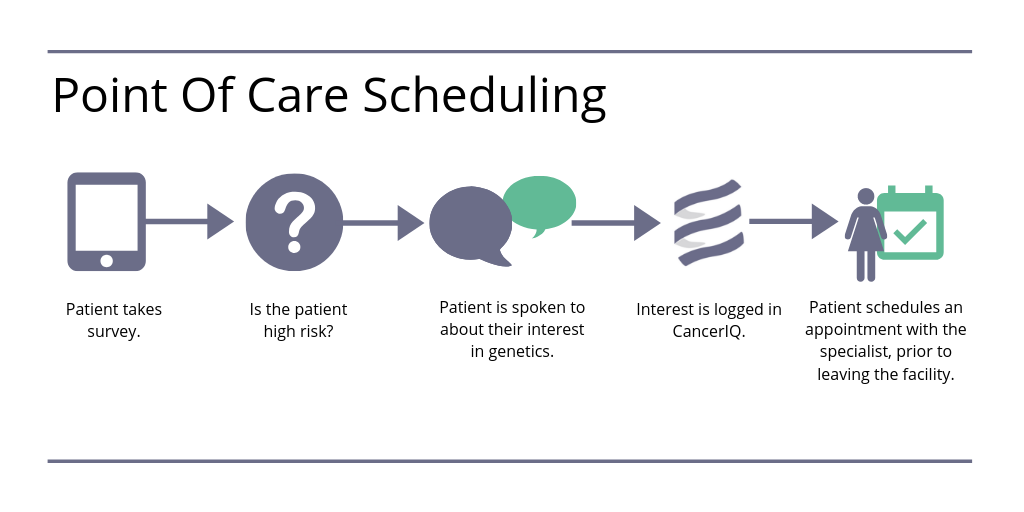
(2) The point of care scheduling model. The screening site makes an appointment with a genetic specialist for all high-risk patients who are interested before the patient leaves the facility.
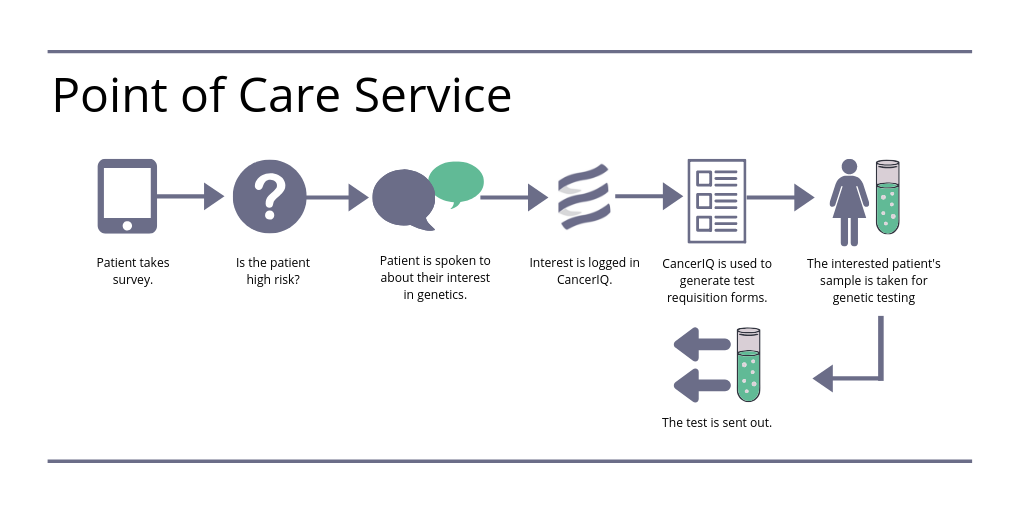
(3) Point of care service model. In this model, all patients who are high risk and interested in genetics will receive genetic counseling and testing at the screening site immediately before leaving the facility.
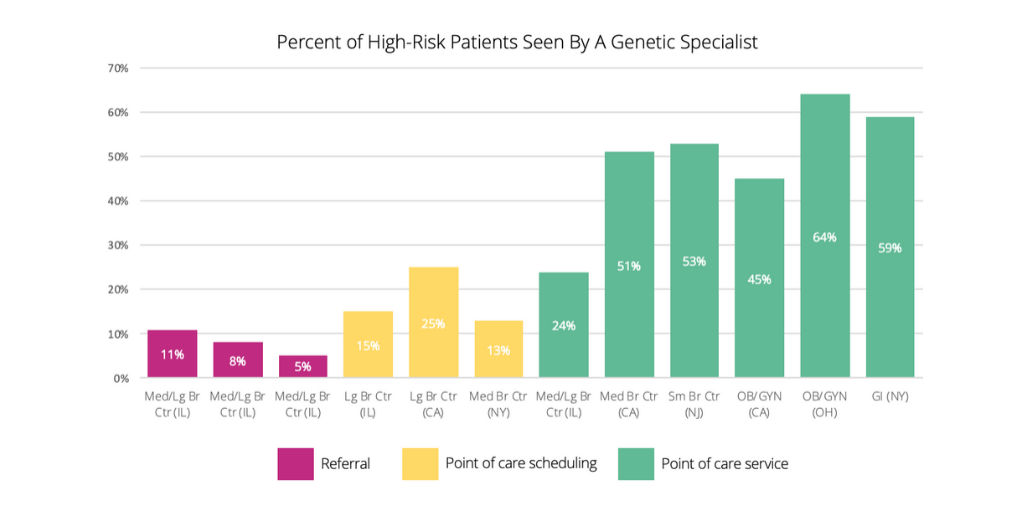
The study examined 12 existing sites across several states that included small to large breast centers, OB/GYN clinics, and a gastrointestinal (GI) location. The researchers looked at how implementation models impacted the number of patients who were actually seen by a genetic counselor. Within that sample, on average:
- 49 percent of patients in the point of care service model saw a genetic counselor.
- 18 percent of patients in the point of care scheduling model saw a genetic counselor.
- 8 percent of patients in the referral model saw a genetic counselor.
How to Increase Patient Uptake to Your Genetic Services
How do these data points translate into actionable insights for your cancer risk assessment program?
By limiting the number of points in your high-risk program where the patient has to make a decision, you may see an increase in uptake of genetic services. In other words, the fewer decision points you make your patients go through, the lower your drop-off rates will be.
With the point of care service model, because the patient decides immediately to see a genetic counselor and get testing before leaving the facility, there is only one decision point that exists. Whereas the referral model has many decision points leading up to genetic counseling and testing, with more time between those decisions, and with more administrative work (e.g., follow-up phone calls) to schedule the patient's appointment with the genetic specialist. Point of care scheduling falls in the middle; it has two decision points: (1) scheduling the patient on the spot and (2) having the patient come back for testing.
Building The Right Implementation Model For Your Risk Assessment Program
How you implement your cancer risk assessment program can significantly impact your overall outcomes.
Generally, risk assessment programs will share some similarities, including:
- The patient completes a screening questionnaire by paper, tablet, or ahead of time.
- The staff reviews the patient results using screening guidelines or software analysis to identify patients who are eligible for genetic counseling and testing.
- Genetics is discussed with patients who are flagged as high risk. (Though it may vary by site, typically the discussion is with the mammography tech, healthcare provider, medical assistant, or mid-level practitioner.)
- The patient indicates interest in genetics, or lack thereof, and it gets logged.
But as the observational study demonstrated, the way you implement you cancer risk assessment and genetics program impacts the number of patients who follow through with your services.
Point of care service has the highest patient uptake compared to the other models. However, it may be more difficult to implement, as it requires strong coordination between scheduling and the genetic specialist’s availability.
The referral model is very easy to implement, because all you need is the screening questionnaire. That said, it also has the lowest effectiveness for achieving patient uptake. And because risk assessment program success depends on how many identified patients are seen by your genetic specialist, the ease of implementation isn’t helping you drive greater patient access.
If you’re currently in the referral model or just starting your program, point of care scheduling is a good place to start while your institution works toward a point of care service model. Point of care scheduling is relatively easy to implement if your genetic specialist's schedules can be shared. As well, it demonstrates a higher patient uptake compared to the referral model.
Overall, though, the availability of staff and number of personnel may limit your choices for the type of implementation model that’s right for your program, and may even prevent you from using the point of care scheduling model. Each institution will be different.
Learn More
Interested in learning which implementation model is right for you? Watch the on-demand webinar "How to Implement Cancer Risk Assessment in your Health System."