Let's face it. The majority of genetics practices are dealing with big problems when it comes to clinical workflow.
It takes a village within a local healthcare system to implement a plan that both manages and navigates high-risk patients to the right experts. In an ideal world, all physicians would keep up with the NCCN guidelines, asking patients the right family history questions and identifying all possible cases of hereditary cancer risk.
Unfortunately, that’s not the always the case.
To ensure a strong referral base and steady stream of patients you need to provide physicians with straightforward education and a screening framework. In this article, we provide three tools to help your referring physicians easily identify patients at risk of Hereditary Breast and Ovarian Cancer (HBOC).
1. Make it Easy for Busy Physicians To Educate Their Patients
The U.S. Preventative Services Task Force (USPSTF) recommends primary care physicians screen all women with a family history of cancer.¹ You know that early detection and a managed care plan can decreases the future impact of hereditary cancer symptoms.
There are easy warning signs for hereditary cancer, and physicians just need the short and accessible information to make that connection.
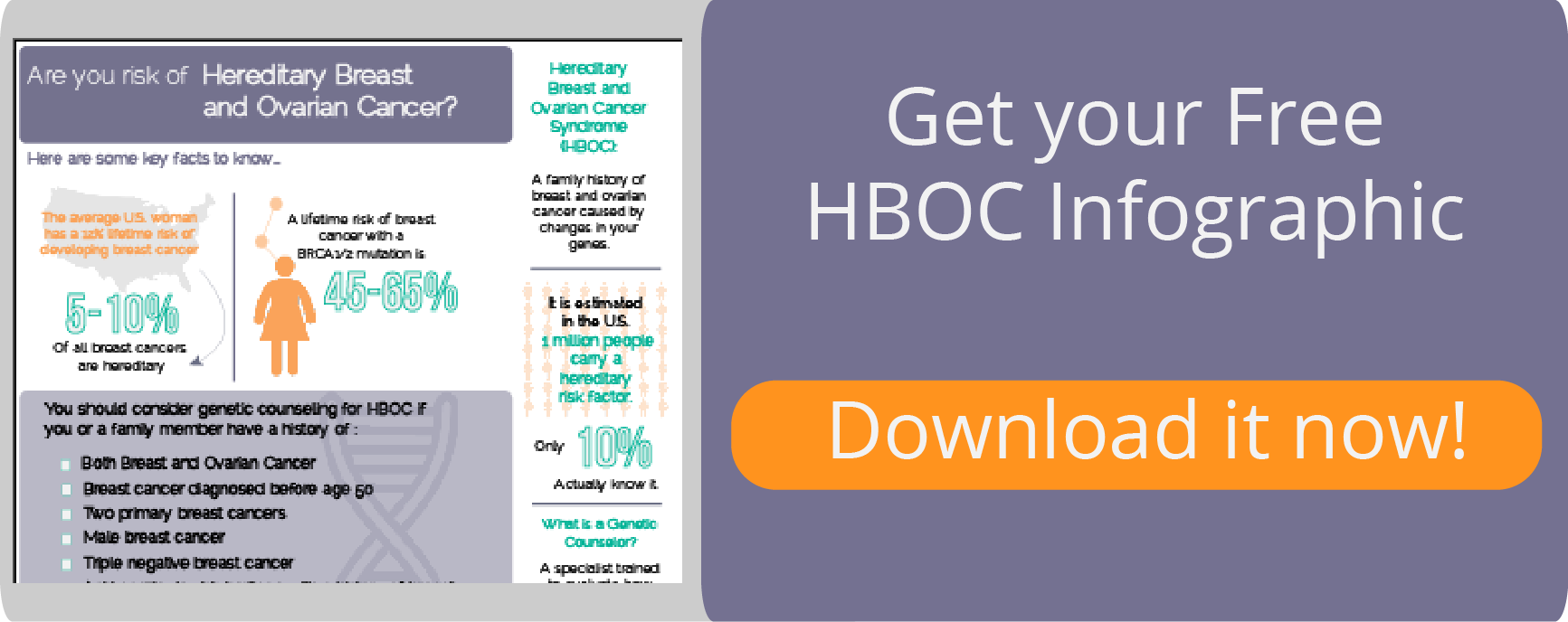
The infographics below can be used in the waiting room or exam room. Most importantly, it can help start a conversation about the patient’s family history and risk factors that can contribute to HBOC Syndrome.
Click here to download a beautiful infographic that physicians can share with their patients:
2. Help Referring Physicians Ask The Right Questions
Genetic counselors have been gathering family history for decades in order to identify high-risk patients.
But when family history gathered by referring physicians is not used to screen and refer high-risk individuals to genetic counseling, patients can fall through the cracks. In a study by the American Society of Clinical Oncology, it was found that a cancer center only had 69% of it’s patient’s family history information in medical records.²
Many of your referring physicians may not have a streamlined system to uncover a patient’s family history and identify those at high risk.
The USPSTF has seven basic questions that physicians can ask to determine high-risk patients.
Click here to download this easy checklist to share with your referring physicians:
These questions can be printed out for patients to complete before the appointment, or asked by a nurse or physician in the exam room. If a patient answers “Yes” to any of the questions, they qualify for a genetic counselor referral.
While it’s not an in-depth screening, it asks the basic questions that physicians may not be aren’t currently asking.
3. Help Referring Physicians Screen Effectively
We know that physicians don’t struggle with technology and spend much of their day working within an EMR. However, they do struggle to keep up with constantly changing screening guidelines.
In the last few years, multiple organizations have published their own guidelines for the age and frequency of mammography screening. Leading physicians to wonder which are correct.
In 2010, The Society of Breast Imaging released that women at average risk should begin annual mammograms at age 40.³ Later in 2015, The American Cancer Society recommended annual mammograms at age 45 and biannual at age 55.4 As of January 2016, USPSTF recommends women with a family history of cancer begin mammogram screenings at age 40.5 This was a change from the 2009 USPSTF recommendation that all women age 50-74 should have biannual mammograms. 6
Referring physicians need a solution that takes out the guesswork and navigates the right patients to the right screening recommendations according to the current guidelines.
How Can CancerIQ Help?
CancerIQ is a digital cancer risk assessment tool that referring physicians can use to identify high-risk patients. The goal of the screening tool is to find patients who may be at risk for developing certain types of hereditary cancer, and to navigate the patients to an individualized plan. This is done while seamlessly integrating into any clinic's workflow.
Patients can complete a short assessment on a tablet in the waiting room or in the exam room while waiting for the physician. Once completed, the patient and physician are alerted of the patient’s risk profile and the recommended next steps- such as booking an appointment with a genetic counselor.
This gives the physician a better picture of the patient’s risk, and streamlines high-risk patients to your practice.
Below is a link for a FREE CancerIQ digital screening questionnaire that you can provide for referring physicians, or for your own practice.

1. Virginia A. Moyer, MD, MPH. Risk Assessment, Genetic Counseling, Genetic Testing for BRCA-related Cancer in Women: U.S. Preventive Services Task Force Recommendation statement For Ann Intern Med. 2014;160(4):271-281
2. J Clin Oncol 20:528-537. © 2002 by American Society of Clinical Oncology.
3. J Am Coll Radiol. 2010 Jan;7(1):18-27. doi: 10.1016/j.jacr.2009.09.022
4. JAMA. 2015 Oct 20;314(15):1599-614. doi: 10.1001/jama.2015.12783
5. U.S. Preventative Services Task Force 2016 January: Final Recommendation Breast Cancer: Screening
6. U.S. Preventative Services Task Force 2009 November: Final Recommendation Breast Cancer: Screening